Discussion
Although GTN is thought to be highly chemosensitive
tumor with very good prognosis, same may not
be always true for ultrahigh risk GTN with brain and
liver metastasis. Ultrahigh risk GTN particularly with
non-molar antecedent pregnancy, brain metastases, and
previous multi-agent chemotherapy failure are poor
prognostic factor.
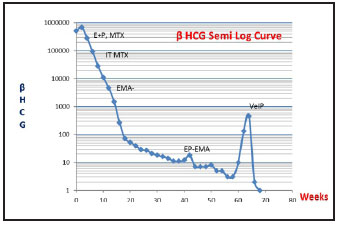
It has been seen that induction with low dose EP
has may reduce the early mortality. EMA/CO can still be
considered as effective regimen and manageable
toxicities for most of the patients with ultrahigh risk
GTN.3 EP-EMA regimen is used in patients who
experienced relapse or became refractory to EMA-CO
treatment.4 In patient with brain metastasis may require
WBRT and/or IT methotrexate (MTX). Salvage
surgeries like hepatic resection, arterial embolization,
stereotactic radiosurgery of cerebral metastasis,
thoracotomy may improve prognosis. Recent studies has
shown that PD1 inhibitors like Pembrolizumab can be
one of the option to treat multi drug resistant ultrahigh
risk GTN but needs more data to establish it as a standard
treatment.5
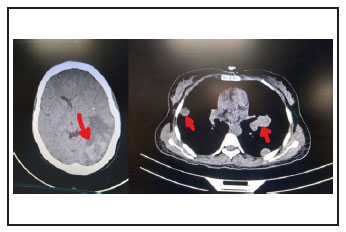
In our case young patient with a small child
having GTN stage IV, WHO score 14 with liver, lung,
brain metastasis was not only traumatizing to the family
but it was a clinical challenge also. At first diagnose the
case as Astrocytoma by outside Neurophysician just
depending upon her neurological symptoms and brain
imaging created confusion. Here lies the importance of
obstetric and gynecologic history for every woman
otherwise recent history of molar pregnancy abortion
would have guided towards GTN from the time of
presentation. Multidisciplinary team work, good patient
compliance, family and financial support which are the
cornerstone for long duration of successful treatment.
Conclusion
Every case of ultrahigh risk of GTN is unique
and very demanding - requiring individual patient
treatment plan according to the clinical scenario and
disease distribution. For each such patient the treating
onco-physician needs some extra devotion to the patient
and very close monitoring to combat the complications
at the earliest. Sometimes multiple chemo resistant or
refractory cases may warrant to even use some
experimental treatment regimen. As there is no standard
treatment for ultrahigh stage of GTN for rarity of the
disease incidence; there should be multi centric
international patient database and clinical study to
establish evidence based management protocol in near
future.
Conflict of Interest
Patient’s consent was procured. There is no
conflict of interest for publication of this case report.
References
1. Kong Y, Yang J, Jiang F et al: Clinical characteristics
and prognosis of ultrahigh-risk gestational
trophoblastic neoplasia patients: a retrospective
cohort study. Gynecologic Oncology 2017;146:81-
86
2. Oranratanaphan S, Lertkhachonsuk R: Treatment of
extremely high risk and resistant gestational
trophoblastic neoplasia patients in King
Chulalongkorn Memorial Hospital. Asian Pacific
Journal of Cancer Prevention 2014;15:925-928
3. Shen T, Chen LL, Qin JL et al: EMA/CO regimen for
chemotherapy 24 patients with ultrahigh-risk
gestational trophoblastic neoplasia. Zhonghua fu
Chan ke za zhi 2018;53:371-376
4. Mao Y, Wan X, Lv W et al: Relapsed or refractory
gestational trophoblastic neoplasia treated with the
etoposide and cisplatin/etoposide, methotrexate, a n
d a c t i n o m y c i n D ( E P - E M A ) r e g i m e n .
International Journal of Gynecology & Obstetrics
2007 ;98:44-47
5. Cheng HY, Yang JJ, Zhao J et al: Preliminary study
of PD-1 inhibitor in the treatment of drug-resistant
recurrent gestational trophoblastic neoplasia.
Zhonghua fu Chan ke za zhi 2020;55:390-394