Discussion
Steroid cell tumour ovary was first described
by Scully.1 Formerly they were referred to as lipid cell
tumours of the ovary. The incidence of a steroid cell
tumours is less than 0.1% of all ovarian tumours.1
Most commonly they present in the childbearing age
group or third and fourth decade of life and very rarely
do they occur in postmenopausal women. These
tumours are hormone secreting and hence cause
androgenic manifestation.
These tumours generally present with
symptoms of virilisation and menstrual irregularity
and hence patients with such symptoms should be
suspected of having adrenal and ovarian tumour
which should be ruled out clinically. In cases of rapid
onset hirsuitism and virilisation, serum testosterone
value above 200 ng/dL is important in diagnosing
neoplastic source of hirsuitism. It is also useful in post
treatment follow up of patients if initially elevated.
Our patient had a proliferative endometrium on
endometrial biopsy. This along with her history of
post-menopausal bleeding indicates an oestrogen
secreting tumour. Hyperestrogenemia presenting as
menorrhagia or post-menopausal bleeding has been
reported in 6 to 23% of women.1 In most of the cases,
the diagnosis of steroid cell tumours- NOS is made
post operatively.
Majority of steroid cell tumours-NOS are
unilateral, solid and well circumscribed with size
ranging from 1.2 to 45 cms.1 Grossly a combination of
solid cystic tumours have also been reported however
purely cystic tumours are extremely rare. Cut surface
range from yellow to orange to red or brown
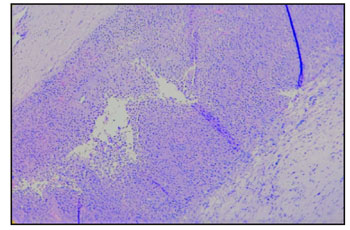
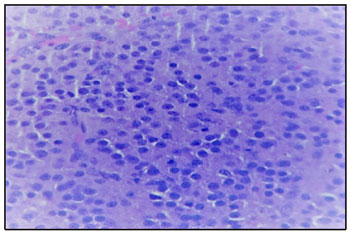
depending on the lipid content.1,2 Microscopically the
tumour cells are polygonal and have abundant
cytoplasm that ranges from eosinophilic (lipid-poor)
to pale and vacuolated (lipid-rich), arranged in sheets
with prominent central nucleus and centrally placed
round nuclei. Immunohistochemistry for inhibin,
calretin and melan A are sensitive markers for steroid
cell tumours- NOS.3
The tumour in our case was solid cystic mass of 7x6 cm, with cut surface showing yellow colour
with areas of necrosis and haemorrhage. Clinico
pathologic correlation is essential for management of
these cases. Treatment of these tumours are based on
histological picture, surgical staging and patients
desire to preserve fertility. As our patient was
postmenopausal, we did a complete staging surgery.
Clinico pathologic parameters which
correlate with malignant behaviour of these tumours
include advanced age at the time of presentation, size
of tumour of 7 cm or more (78%), mitotic figures
more than 2 / 10 hpf (92%), grade 2 to 3 nuclear atypia
(64%), presence of necrosis (86%) and haemorrhage
(77%). 1,4
In the present case even though the patient
had adverse prognostic factors like older age at
presentation, increased mitotic rate, size of the tumour
of 7 cm and presence of necrosis and haemorrhage, the
patient has been kept on close observation as she has
undergone an optimal staging surgery and FIGO stage
of tumour being IA. Patient is disease free till date.
Conclusion
Steroid cell tumours-NOS are very rare
ovarian sex cord stromal tumours which usually
present with varied symptoms like menstrual
irregularities, hirsutism and abdominal pain. In
postmenopausal women therapeutic complete surgery
should be performed. Clinical correlation along with
histopathologic examination is the gold standard that
can confirm the diagnosis in most cases and in atypical
cases immunohistochemistry plays a very significant
role.
References
1. Hayes MC, Scully RE: Ovarian steroid cell
t u m o u r s ( n o t o t h e r w i s e s p e c i f i e d ) . A
clinicopathological analysis of 63 cases. Am J
Surg Pathol 1987;11:835-845
2. Outwater EK, Wagner BJ, Mannion C et al: Sex
Cord-stromal and steroid cell tumours of the
ovary. Radio graphics 1998;18:1523-1546
3. Kurman RJ: International Agency for Research on
Cancer, and World Health Organization, WHO
classification of tumours of female reproductive
organs, International Agency for Research on
Cancer, Lyon, 4th edition, 2014, World Health
Organization classification of tumours.
4. RubidoValle CD, Fuentes JL, Martinez CS et al:
Ovarian steroid cell tumour associated to
endometrial hyperplasia and presenting as post
menopausal vaginal bleeding. Gynecol Obstet
2015;5:316
5. Sawathiparnich P, Sitthinamsuwan P, Sanpakit K:
Cushing’s syndrome caused by ACTH- producing
ovarian steroid cell tumour, NOS, in a prepubertal
girl. Endocrine 2009;35:132-135